The United States is currently grappling with a public health emergency of unprecedented proportions, characterized by a staggering rise in drug overdose deaths primarily driven by opioids. What began in the late 1990s as a surge in prescription-related dependencies has evolved into a multi-faceted crisis involving heroin and highly potent synthetic opioids like fentanyl. According to data from the Centers for Disease Control and Prevention (CDC) and the United Nations Office on Drugs and Crime (UNODC), the American opioid epidemic is not merely a domestic issue but a global outlier in terms of lethality and the speed of its escalation. Investigative efforts, such as the Pulitzer Prize-winning report "Seven Days of Heroin" by the Cincinnati Enquirer, have documented the granular devastation of this crisis, revealing that in a single week, a single metropolitan area can witness hundreds of overdoses and dozens of fatalities. This reality has prompted data scientists and public health officials to look beyond anecdotal evidence and utilize comprehensive datasets to understand the underlying patterns of addiction, mortality, and regional vulnerability.
The Three Waves of the Opioid Epidemic
To understand the current state of the crisis, it is essential to examine the chronological progression of the epidemic, which public health experts categorize into three distinct waves. The first wave began in the late 1990s, following the increased prescription of opioids for pain management. Pharmaceutical companies reassured the medical community that patients would not become addicted to prescription opioid pain relievers, leading healthcare providers to prescribe them at greater rates. This widespread availability led to high rates of diversion and misuse before the addictive nature of these medications was fully recognized.
The second wave began in 2010, marked by a rapid increase in overdose deaths involving heroin. As authorities began to crack down on "pill mills" and the over-prescription of painkillers, individuals who had become dependent on prescription opioids transitioned to heroin, which was often cheaper and more readily available on the black market. The third wave, which began around 2013, is characterized by a significant spike in deaths involving synthetic opioids, particularly illicitly manufactured fentanyl. Fentanyl is 50 to 100 times more potent than morphine and is often mixed into heroin, cocaine, and counterfeit pills, frequently without the user’s knowledge. This third wave has proven to be the most lethal, as even minute quantities of the substance can cause a fatal respiratory arrest.
Comparative Analysis of Drug Usage and Lethality
When examining data regarding drug use by age, a striking disparity emerges between the prevalence of use and the rate of mortality. Data compiled by FiveThirtyEight and the Substance Abuse and Mental Health Services Administration (SAMHSA) indicates that while marijuana and alcohol remain the most widely used substances across almost all age demographics, heroin and synthetic opioids carry a disproportionately high risk of death. For instance, in the 20-34 age demographic, heroin usage rates are statistically lower than those for cocaine or hallucinogens. However, the lethality of heroin and its synthetic counterparts means that this smaller user base accounts for a majority of drug-induced fatalities.
The data suggests that heroin is particularly concentrated among young adults, whereas substances like crack and cocaine show a more distributed adoption among older age groups. This concentration in the 20-34 demographic highlights a "lost generation" risk, where the most productive years of an individual’s life are cut short by a substance that offers very little margin for error. Unlike other substances where chronic use leads to long-term health decline, the primary risk of opioid use is acute toxicity, leading to immediate death.
The United States as a Global Outlier
A comparative analysis of international data from the UNODC reveals that the United States leads the world in overdose deaths, both in absolute numbers and when adjusted per million inhabitants. While the opioid crisis is often discussed as a general Western phenomenon, the statistics show a significant gap between the U.S. and its peers. Countries like Sweden, Australia, and Canada have reported rising rates of opioid-related issues, yet their death rates remain less than half of those recorded in the United States.
Iceland presents a unique statistical outlier; due to its very small population, a relatively low number of absolute deaths (approximately 45 in certain reporting years) results in a high death-per-million ratio. However, when looking at large-scale industrial nations, the U.S. remains at the epicenter. Several factors contribute to this American exceptionalism in drug mortality, including the privatized nature of the healthcare system which historically incentivized the prescription of pills over physical therapy or long-term counseling, as well as a lack of centralized drug monitoring systems during the early stages of the epidemic.
Regional Hotspots and Domestic Trends
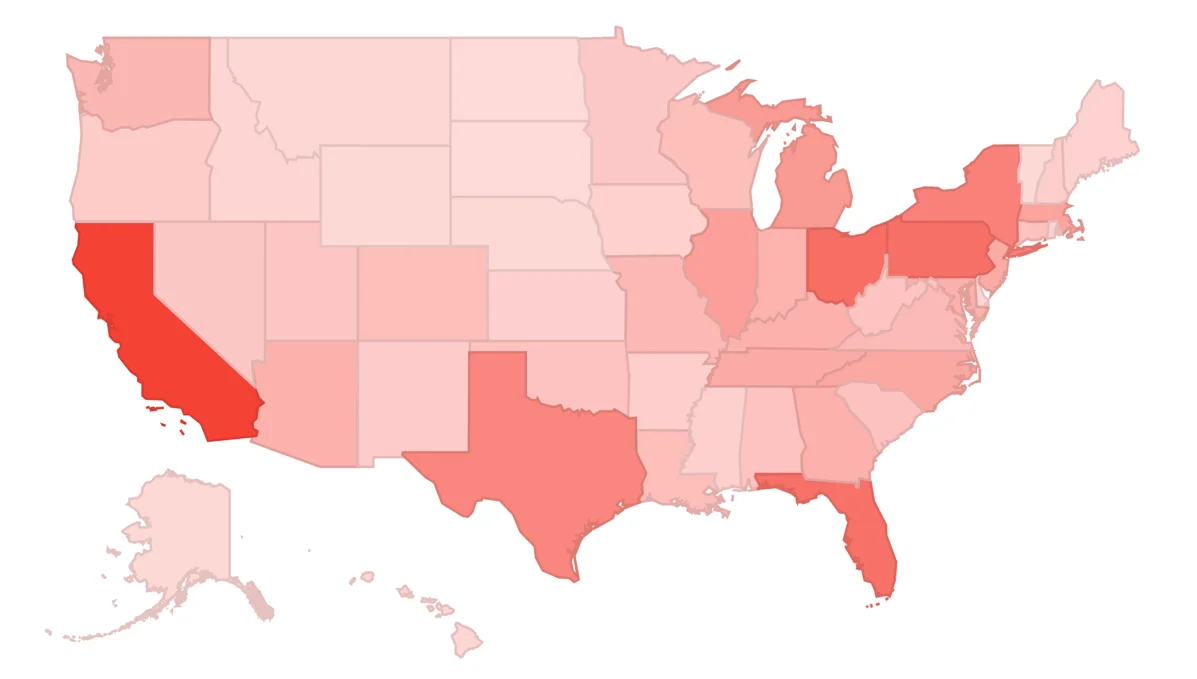
Within the United States, the epidemic does not impact all regions equally. Data from the CDC’s National Center for Health Statistics shows that the Appalachian region, the Rust Belt, and parts of New England have been hit hardest. States like West Virginia, Ohio, and New Hampshire consistently report the highest rates of overdose deaths per 100,000 residents. In these areas, the crisis is often intertwined with economic decline, the loss of manufacturing jobs, and a lack of access to comprehensive mental health services.
However, the trend is shifting. While the crisis was initially identified as a rural or "blue-collar" problem, data now shows a rapid increase in overdose deaths in urban centers and among diverse demographic groups. The influx of fentanyl into the cocaine and methamphetamine supply has expanded the victim profile beyond those traditionally seeking opioids. Analysts monitoring these trends use data visualization tools to identify "hot zones" where emergency services and Narcan (naloxone) distribution should be prioritized. The ability to track these developments in real-time is crucial for local governments to allocate resources effectively.
Official Responses and Legal Implications
The scale of the crisis has triggered significant responses from the federal government and the legal system. In 2017, the U.S. Department of Health and Human Services (HHS) declared the opioid crisis a public health emergency. This declaration allowed for the redirection of federal resources and the expansion of access to medication-assisted treatment (MAT), such as buprenorphine and methadone.
Simultaneously, a wave of litigation has targeted the pharmaceutical industry. Thousands of lawsuits have been filed by states, cities, and Native American tribes against manufacturers like Purdue Pharma, distributors like AmerisourceBergen, and retail pharmacies like CVS and Walgreens. These legal actions allege that companies downplayed the risks of addiction and failed to monitor suspicious orders of narcotics. Recent settlements have reached into the tens of billions of dollars, with the funds earmarked specifically for addiction treatment and prevention programs. This represents one of the largest legal reckonings in corporate history, drawing parallels to the Big Tobacco settlements of the 1990s.
The Role of Data in Shaping Solutions
The transition from viewing addiction as a moral failing to treating it as a chronic medical condition has been heavily influenced by data-driven insights. By analyzing datasets from the CDC and UNODC, researchers can identify which interventions are most effective. For example, data shows that states with robust prescription drug monitoring programs (PDMPs) and expanded access to naloxone have seen a slower rate of increase in overdose deaths compared to those without such measures.
Furthermore, data visualization has become an essential tool for public communication. When complex statistics are translated into interactive maps and charts, the immensity of the problem becomes tangible for policymakers and the general public. This transparency is vital for maintaining the political will necessary to fund long-term recovery initiatives. Analysts are now calling for more granular data, including real-time emergency room reporting and wastewater testing, to stay ahead of the evolving chemical compositions of illicit drugs.
Broader Socioeconomic Impact and Future Outlook
The implications of the opioid epidemic extend far beyond the healthcare sector. The economic burden is estimated to be over $1.5 trillion annually, accounting for healthcare costs, lost productivity, and the strain on the criminal justice system. Additionally, the crisis has placed an immense burden on the foster care system, as tens of thousands of children are displaced due to parental substance use disorders or fatal overdoses.
Looking forward, the path to mitigation requires a multi-pronged approach that combines aggressive law enforcement targeting fentanyl supply chains with compassionate, evidence-based treatment for those already suffering from dependency. The "Seven Days of Heroin" report served as a wake-up call, showing that the crisis is not a distant statistic but a daily reality for thousands of families. As the United States continues to battle this epidemic, the integration of data science and public health policy will remain the most effective weapon in identifying trends, preventing new cases of addiction, and ultimately saving lives. The challenge lies in maintaining a sustained response that matches the scale of the data, ensuring that the lessons learned from the three waves of the crisis are used to prevent a fourth.