The United States is currently grappling with one of the most devastating public health crises in its history, characterized by a staggering rise in drug overdose deaths driven primarily by opioids. What began in the late 1990s as a surge in prescription drug misuse has evolved into a multi-faceted epidemic involving heroin and, most recently, highly potent synthetic opioids like fentanyl. According to data from the Centers for Disease Control and Prevention (CDC) and the United Nations Office on Drugs and Crime (UNODC), the American opioid crisis represents a unique anomaly in global health, with mortality rates that far exceed those of other developed nations. To understand the depth of this crisis, analysts have turned to comprehensive datasets to track trends, identify demographic vulnerabilities, and map the geographic spread of a phenomenon that claims tens of thousands of lives annually.
A Chronology of Addiction: The Three Waves of the Epidemic
The trajectory of the US opioid crisis is generally categorized by public health experts into three distinct waves, each defined by the primary substance driving mortality rates. Understanding this chronology is essential for contextualizing how the current state of emergency reached its present proportions.
The first wave began in the 1990s, following the increased prescription of opioids for the treatment of chronic pain. Pharmaceutical marketing campaigns, most notably those surrounding OxyContin, assured the medical community that the risk of addiction was low. This led to a massive influx of prescription opioids into American households. By the time the addictive potential of these drugs was fully realized, a significant portion of the population had already developed a dependency.
The second wave emerged around 2010, characterized by a rapid increase in overdose deaths involving heroin. as authorities began to tighten regulations on prescription opioids and “pill mills,” individuals who had become addicted to prescription pills turned to heroin as a cheaper and more accessible alternative. The transition from the medicine cabinet to the street marked a turning point where the crisis became more lethal and harder to contain.
The third and most current wave began in 2013, with a significant spike in deaths involving synthetic opioids—particularly illicitly manufactured fentanyl. Fentanyl, which can be 50 to 100 times more potent than morphine, is often mixed into heroin, cocaine, and counterfeit pills, often without the user’s knowledge. This has led to a dramatic escalation in the lethality of drug use, as even a microscopic dose can be fatal.
Global Perspectives and Comparative Mortality Rates
When placed in a global context, the United States remains an extreme outlier regarding drug overdose deaths. Data from the UNODC indicates that while drug use is a universal issue, the United States leads the world in both absolute overdose numbers and deaths per million people. In many European and Asian nations, drug policies emphasize harm reduction and strict pharmaceutical controls, which has resulted in significantly lower mortality rates despite similar levels of recreational drug use.
For instance, while countries like Sweden and Australia report high rates of drug-related deaths per capita relative to their neighbors, their rates remain less than half of those seen in the United States. Iceland occasionally appears as a statistical outlier in global data due to its very small population; a handful of deaths can result in a high per-million figure, yet the absolute scale of the problem there does not compare to the systemic crisis in the US.
In the United States, the overdose death rate has frequently surpassed the mortality rates of automobile accidents and firearm-related incidents, becoming a leading cause of death for adults under the age of 50. This disparity highlights a specifically American problem rooted in healthcare delivery, the history of pharmaceutical regulation, and the socio-economic factors that drive substance use disorders.
Demographic Shifts and the Lethality of Synthetic Opioids
Analysis of drug use by age, utilizing data from sources such as FiveThirtyEight and the CDC, reveals surprising patterns regarding who is most at risk. While drugs like cocaine and crack show a broad distribution of use among older age groups (35-60+), heroin and synthetic opioid use is more concentrated among younger demographics, particularly those aged 20 to 34.
The data suggests a grim reason for this concentration: the lethality of the drug. Because heroin and fentanyl have such high overdose rates, there is a “survivorship bias” in the data. Users of less lethal stimulants may continue use into their 50s and 60s, whereas opioid users face a much higher probability of a fatal encounter before reaching middle age. Furthermore, the rapid onset of the synthetic opioid wave has meant that many new users are dying much earlier in their journey of addiction than previous generations did with prescription pills or pure heroin.
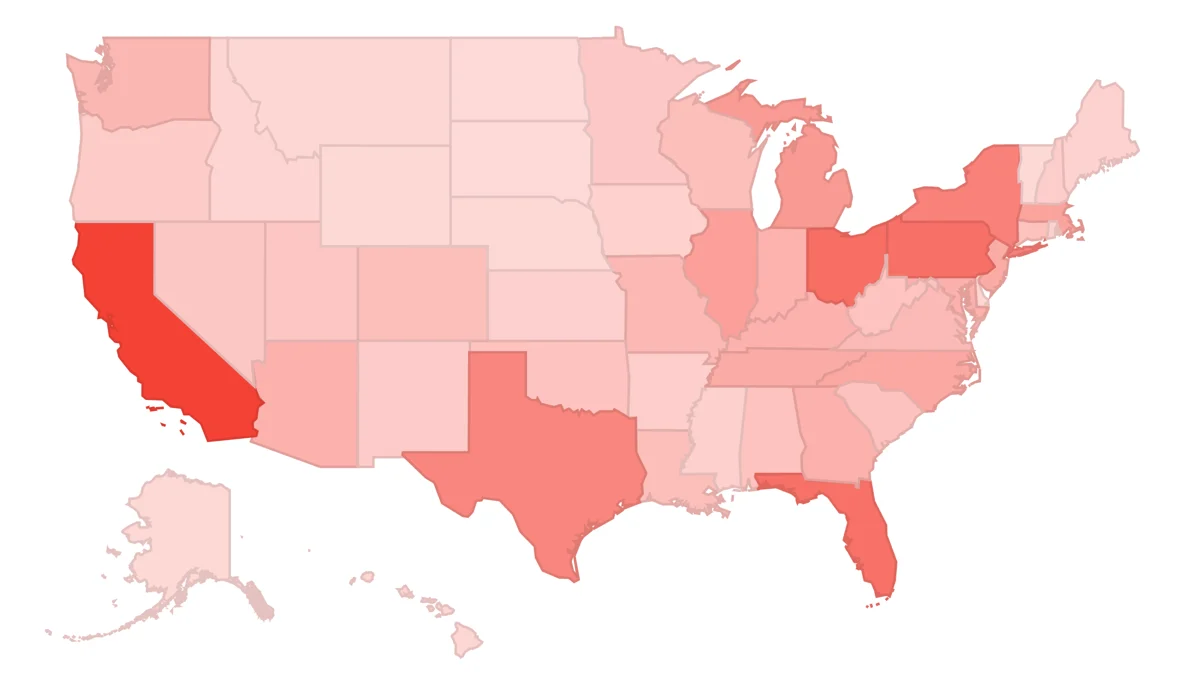
Regional Disparities and State-Level Impact
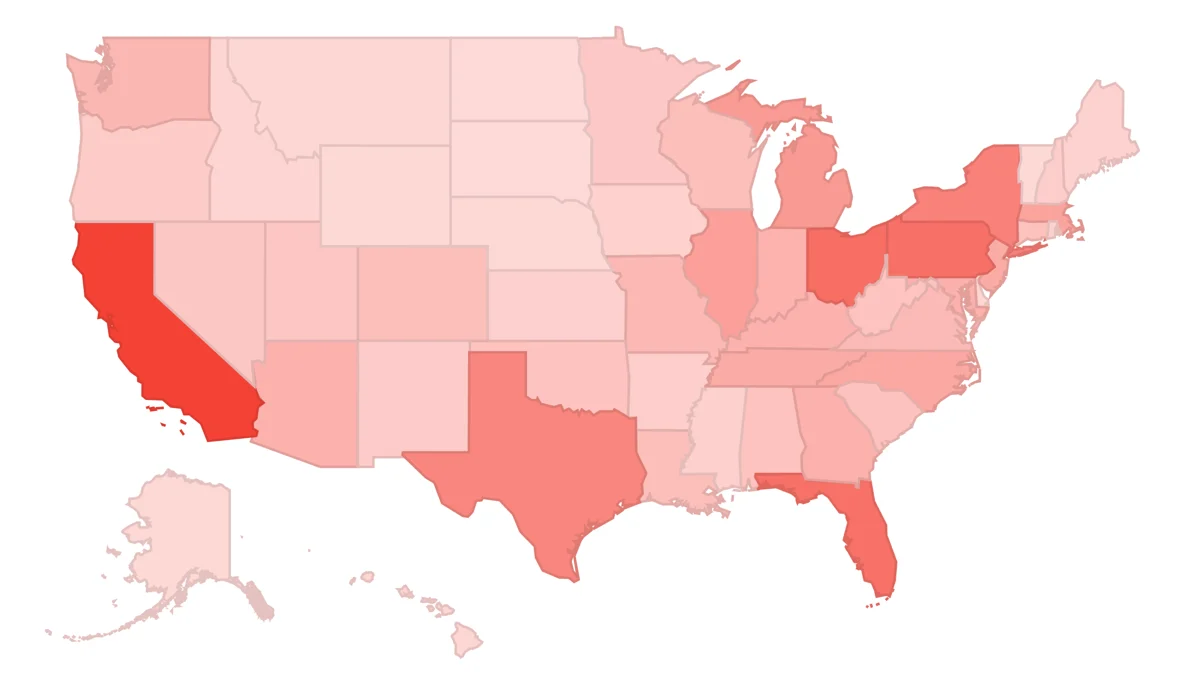
The opioid epidemic has not affected all parts of the United States equally. Data visualizations of CDC death rates show a concentrated “overdose belt” stretching through the Appalachian region and into the Midwest. States such as West Virginia, Ohio, and Pennsylvania have consistently reported the highest rates of overdose deaths per 100,000 residents.
West Virginia, in particular, has become the epicenter of the crisis. Economic stagnation in former coal-mining communities, combined with high rates of workplace injuries and subsequent over-prescription of painkillers, created a “perfect storm” for addiction. Conversely, states with more robust social safety nets or different prescribing cultures, such as those in the Great Plains or parts of the Northeast, have seen different trend lines, though no state has been entirely spared.
In recent years, the crisis has shifted geographically. While the East Coast was initially hit hardest by the influx of fentanyl, Western states that previously saw lower rates are now seeing rapid increases. This suggests that the supply chains for synthetic opioids are becoming more sophisticated and pervasive, reaching markets that were once insulated from the worst of the epidemic.
Public Health Responses and Legislative Action
The scale of the crisis has forced a shift in how the US government and legal systems approach drug addiction. For decades, the “War on Drugs” focused primarily on criminalization and incarceration. However, the current epidemic has prompted a move toward a public health model.
-
Litigation against Pharmaceutical Companies: In a series of landmark legal battles, states and municipalities have sued major pharmaceutical manufacturers and distributors, such as Purdue Pharma and Johnson & Johnson. These lawsuits allege that the companies downplayed the risks of opioids and used aggressive marketing tactics to increase sales. Settlements totaling billions of dollars have been earmarked for addiction treatment and prevention programs.
-
Access to Naloxone: Public health officials have prioritized the widespread distribution of Naloxone (Narcan), an opioid antagonist that can reverse an overdose in progress. Many states have passed “Good Samaritan” laws to protect those who administer the drug and have made it available over the counter without a prescription.
-
Medication-Assisted Treatment (MAT): There is a growing consensus among medical professionals that addiction should be treated as a chronic brain disease. Programs utilizing Methadone or Buprenorphine have proven effective in reducing withdrawal symptoms and cravings, allowing individuals to stabilize their lives.
-
Monitoring Programs: Prescription Drug Monitoring Programs (PDMPs) have been implemented nationwide to help doctors identify “doctor shopping” and prevent the over-prescription of narcotics.
The Economic and Social Toll of Prolonged Crisis
Beyond the tragic loss of life, the opioid epidemic has exerted a profound economic and social toll on the United States. The Council of Economic Advisers has previously estimated the annual cost of the crisis to be over $500 billion, factoring in healthcare costs, lost productivity, and the strain on the criminal justice system.
Socially, the crisis has fueled a rise in the number of children entering the foster care system, as parents struggle with addiction or succumb to overdoses. This has created a “lost generation” in the hardest-hit regions, where grandparents are frequently called upon to raise their grandchildren. Furthermore, the epidemic has placed an unprecedented burden on first responders and emergency room staff, many of whom face burnout from the sheer volume of overdose calls they must attend to daily.
Data as a Tool for Future Reform
The journey to understand the opioid crisis through data highlights a critical reality: words and videos can convey the human tragedy, but data provides the map for the solution. By analyzing trends in drug adoption, lethality, and geographic spread, policymakers can better allocate resources to the areas where they are most needed.
The transition from prescription drugs to heroin and finally to fentanyl illustrates the “Whack-a-Mole” nature of drug policy; as one supply is restricted, another, often more dangerous, emerges to fill the void. This underscores the need for a holistic approach that focuses on reducing demand through treatment and addressing the underlying socio-economic drivers of despair.
As analysts continue to peel back the layers of the US opioid epidemic, the data serves as a call to action. The patterns are clear, and the trends are documented. The challenge remains for society to use this information to implement effective, compassionate, and evidence-based interventions that can finally stem the tide of this national emergency. The goal is not merely to understand the numbers, but to ensure that the data eventually reflects a downward trend in lives lost and a rise in communities healed.