The opioid epidemic represents one of the most significant public health challenges of the 21st century, characterized by a staggering increase in drug-related fatalities and a fundamental shift in the landscape of substance abuse. While the crisis has roots in the over-prescription of pain medications in the late 1990s, it has evolved into a multi-faceted emergency involving illicit heroin and highly potent synthetic opioids like fentanyl. For data analysts and public health officials, understanding the trajectory of this epidemic requires a deep dive into comparative global statistics, demographic shifts, and regional trends that define the current state of drug mortality.
The Evolution of the Epidemic: A Chronology of Three Waves
The United States Centers for Disease Control and Prevention (CDC) identifies the opioid crisis as having progressed through three distinct waves. Understanding this chronology is essential to grasping why the current death toll has reached historic highs.
The first wave began in the late 1990s, following the increased prescription of opioids for the treatment of chronic pain. Pharmaceutical marketing campaigns assured the medical community that the risk of addiction was low, leading to a massive influx of prescription opioids into American households. By the time the addictive potential of these substances was fully realized, a significant portion of the population had developed dependencies.
The second wave emerged around 2010, marked by a rapid increase in overdose deaths involving heroin. as access to prescription opioids became more restricted through legislation and prescription monitoring programs, individuals suffering from opioid use disorder transitioned to heroin, which was often cheaper and more readily available on the illicit market.
The third and most lethal wave began in 2013, characterized by the surge in deaths involving synthetic opioids—particularly illicitly manufactured fentanyl. Fentanyl, which is 50 to 100 times more potent than morphine, is frequently mixed into heroin, cocaine, and counterfeit pills, often without the user’s knowledge. This high potency has dramatically decreased the margin for error, leading to the current spike in accidental overdose deaths.
Comparative Global Mortality: The United States as a Statistical Outlier
When examining global data provided by the United Nations Office on Drugs and Crime (UNODC), the United States stands out as a significant outlier in terms of drug-related mortality. While the opioid crisis is often discussed as a domestic issue, international comparisons reveal the unique severity of the American situation.
In absolute numbers and per capita rates, the United States leads the world in overdose deaths. While other nations struggle with substance abuse, the scale of the American epidemic is unparalleled. For instance, while countries like Sweden and Australia report high death rates relative to their neighbors—averaging roughly half the rate of the U.S. per million people—they do not reach the concentrated mortality levels seen in North America.
Iceland presents a unique statistical case. Due to its very small population, a relatively low number of deaths (approximately 45 in a given reporting period) can result in a high per-million mortality rate, making it an outlier in per capita data. However, the systemic nature of the crisis in the U.S. is distinct because it affects a massive, diverse population across a vast geographic area. In the U.S., the crisis is not merely a localized spike but a sustained national emergency that has seen death rates climb steadily for over two decades.
Demographic Vulnerabilities and the Lethality of Heroin
Data from organizations such as FiveThirtyEight and the CDC highlight a troubling discrepancy between drug usage rates and drug lethality. When analyzing drug use by age, researchers have found that while marijuana and alcohol see widespread use across most adult age groups, heroin usage is statistically less common. However, despite having fewer users than many other illicit substances, heroin and synthetic opioids account for a disproportionately high percentage of total drug deaths.
The data indicates that heroin use is most concentrated among the 20-34 age demographic. This concentration may be attributed to several factors, including the high lethality of the drug, which prevents long-term usage patterns seen in "legacy" drugs like cocaine or crack. In contrast, cocaine and crack cocaine show a more distributed adoption rate among older age groups, suggesting that users of these stimulants may survive longer with their addiction compared to those using high-potency opioids.
The extreme lethality of the current drug supply means that the "experimental" phase of drug use is now more dangerous than ever. For the 20-34 age group, the risk of a single encounter with a fentanyl-laced product resulting in death has fundamentally changed the nature of the public health response, shifting the focus from long-term rehabilitation to immediate harm reduction and the distribution of overdose-reversal agents like naloxone.
Regional Hotspots and Domestic Development Trends
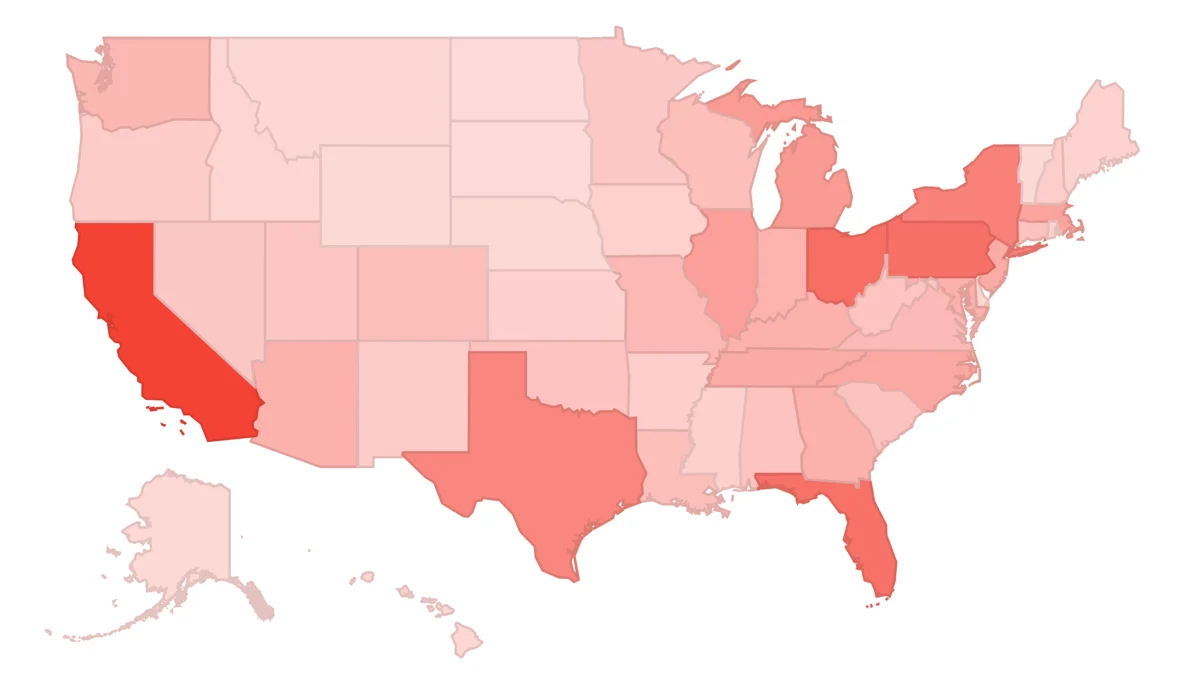
The impact of the opioid epidemic is not uniform across the United States. Regional data reveals specific "hotspots" where the crisis has taken an especially heavy toll, as well as states that are experiencing rapid escalations in mortality.
Historically, the Appalachian region—including states like West Virginia, Ohio, and Kentucky—has been the epicenter of the crisis. These areas were hit hard by the first wave of prescription opioid over-distribution, exacerbated by economic downturns and a lack of access to comprehensive healthcare. West Virginia, in particular, has consistently reported the highest overdose death rates in the nation.
However, recent trends show the crisis expanding into New England and the Southwest. States like New Hampshire and Massachusetts have seen dramatic increases in fentanyl-related deaths. Conversely, some states have shown more resilience or have implemented more successful intervention strategies, resulting in slower growth rates of overdose fatalities. Analyzing these "development trends" allows policymakers to identify which state-level interventions—such as expanded Medicaid, supervised injection sites, or aggressive prescription monitoring—are most effective at curbing the tide of deaths.
Institutional Responses and Official Perspectives
The response from federal and international agencies has been multifaceted, focusing on law enforcement, medical regulation, and public health. The Drug Enforcement Administration (DEA) has focused on disrupting the supply chains of precursor chemicals used to manufacture fentanyl, largely originating from overseas.
Simultaneously, the Department of Health and Human Services (HHS) has declared the opioid crisis a public health emergency, a move that has freed up federal funding for addiction treatment and the expansion of the healthcare workforce in rural areas. The CDC has issued revised guidelines for prescribing opioids for chronic pain, urging clinicians to prioritize non-opioid therapies and to prescribe the lowest effective dose when opioids are necessary.
Public health experts emphasize that data transparency is a critical component of the response. By making overdose data available in near-real-time, local health departments can issue "bad batch" alerts to the community, potentially saving lives by warning users of particularly potent substances entering the local market.
Broader Societal Impact and Implications
The implications of the opioid epidemic extend far beyond the healthcare sector. The economic cost of the crisis is estimated to be in the hundreds of billions of dollars annually, accounting for healthcare costs, lost productivity, and the burden on the criminal justice system.
Furthermore, the crisis has had a devastating impact on the American family structure. There has been a documented surge in the number of children entering the foster care system due to parental substance use or overdose. The "grandparent-headed household" has become an increasingly common demographic as the middle generation is decimated by addiction.
From a data-driven perspective, the crisis highlights the necessity of using advanced analytics to predict and prevent future outbreaks of substance abuse. By monitoring search trends, emergency room admissions, and forensic laboratory data, analysts can provide a roadmap for where resources should be deployed.
Conclusion: The Role of Data in Social Betterment
The journey to understand the opioid epidemic through data reveals a grim reality: the United States is facing a mortality crisis of unprecedented proportions. However, the same data that illustrates the tragedy also offers the path to a solution. Through the rigorous analysis of overdose patterns, demographic vulnerabilities, and the efficacy of various treatments, society can move toward more informed, compassionate, and effective interventions.
The call to action for data scientists, analysts, and policymakers is clear. The skills used to track market trends or optimize business workflows must be applied to public health challenges. By transforming raw numbers into actionable insights, the global community can better understand the nuances of addiction and work toward a future where the devastating patterns of the opioid epidemic are finally broken. This is not merely a statistical exercise; it is a fundamental requirement for the preservation of public health and the improvement of societal well-being.